

You feel perfectly fine. Your periods come regularly, your skin is clear, you maintain a healthy weight, and you’ve never struggled with unwanted hair growth. Then during a routine ultrasound or fertility evaluation, your doctor mentions “polycystic ovaries” or suggests PCOS testing. You’re confused—how can you have PCOS when you don’t have any symptoms?
Yes, you can absolutely have polycystic ovary syndrome (PCOS) without experiencing obvious symptoms—a presentation often called “asymptomatic PCOS” or “silent PCOS.” PCOS is a spectrum disorder with extremely variable presentation, meaning some women experience severe, debilitating symptoms while others have such mild manifestations that they remain undiagnosed for years or are discovered only incidentally during testing for other reasons.
This isn’t a rare exception—studies suggest that 20-30% of women with PCOS have minimal symptoms or presentations so subtle they go unnoticed. Understanding asymptomatic PCOS matters because even without visible signs, the condition carries significant long-term health implications that benefit from early intervention.
Table of Contents
What Exactly Is PCOS and How Is It Diagnosed?
Polycystic ovary syndrome is a complex hormonal disorder affecting 8-13% of reproductive-aged women globally, making it the most common endocrine condition in this population. Despite its name, you don’t need to have cysts on your ovaries to have PCOS, and having polycystic ovaries alone doesn’t automatically mean you have the syndrome.
PCOS diagnosis uses Rotterdam Criteria (established 2003)—you need 2 of these 3 features:
- Irregular ovulation or anovulation (absent or infrequent periods)
- Clinical or biochemical signs of hyperandrogenism (excess male hormones—acne, hirsutism, or elevated testosterone in blood tests)
- Polycystic ovaries on ultrasound (12+ follicles per ovary or increased ovarian volume)
According to NIH research on PCOS diagnosis, this creates four distinct PCOS phenotypes, some of which present with minimal symptoms.
The four PCOS phenotypes:
| Phenotype | Irregular Periods | High Androgens | Polycystic Ovaries | Symptom Visibility |
|---|---|---|---|---|
| Type A (Classic) | ✓ | ✓ | ✓ | Very noticeable |
| Type B | ✓ | ✓ | ✗ | Moderate symptoms |
| Type C | ✓ | ✗ | ✓ | Mild symptoms |
| Type D (Ovulatory) | ✗ | ✓ | ✓ | Minimal/subtle |
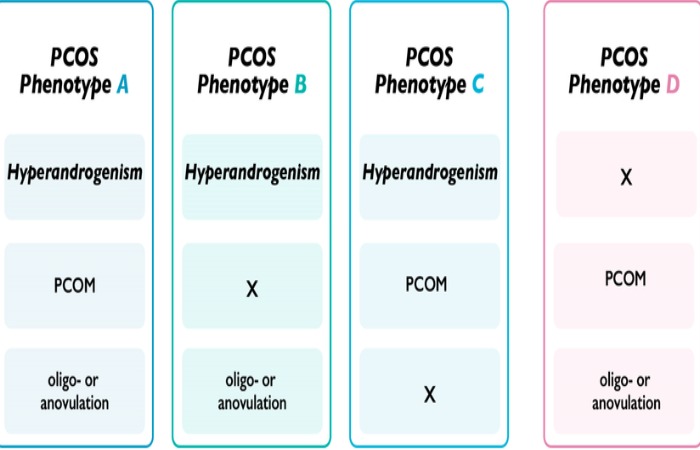
Type D is where asymptomatic PCOS typically falls—women ovulate regularly (normal periods) but have polycystic ovaries and mildly elevated androgens that don’t cause obvious physical manifestations.
Who Has PCOS Without Obvious Symptoms?
Silent PCOS is more common in women who:
- Have regular menstrual cycles (every 21-35 days)
- Maintain normal or lower body weight (lean PCOS affects 20-30% of cases)
- Have mild androgen elevation below the threshold causing visible symptoms
- Come from certain ethnic backgrounds with different symptom expression
- Are discovered during fertility testing (unexplained difficulty conceiving)
- Undergo routine pelvic ultrasounds for other reasons
- Have strong genetic predisposition but mild phenotype expression
Real-world example: A 28-year-old woman with perfectly regular 30-day cycles, clear skin, and normal BMI tried conceiving for 18 months without success. Fertility workup revealed polycystic ovaries on ultrasound and borderline-high testosterone (55 ng/dL; normal <50). She had no classic symptoms but met PCOS diagnostic criteria. After three months of lifestyle modifications and ovulation support, she conceived naturally.
This illustrates a critical point: lack of symptoms doesn’t mean lack of condition or lack of health impact.
Why Some Women Have PCOS Without Noticeable Symptoms
Biological factors explaining asymptomatic presentation:
1. Mild hormonal imbalance Testosterone might be elevated to 52 ng/dL instead of severe elevation to 80+ ng/dL. This subtle increase doesn’t trigger acne or excess hair growth but still disrupts metabolic and reproductive function.
2. Individual androgen sensitivity Some women’s bodies are less sensitive to androgens. Two women with identical testosterone levels might have completely different physical manifestations based on androgen receptor genetics and 5-alpha reductase enzyme activity.
3. Lean PCOS phenotype Women without insulin resistance or obesity often have milder symptoms. Their PCOS is driven more by genetics and ovarian dysfunction than metabolic issues, resulting in subtler presentations.
4. Regular ovulation with polycystic morphology Some women ovulate regularly despite having polycystic-appearing ovaries. Their hormone fluctuations are mild enough not to disrupt cycles but still create ultrasound changes.
5. Compensatory mechanisms The body may compensate effectively for mild hormonal imbalances, masking symptoms while underlying dysfunction persists. Sex hormone-binding globulin (SHBG) might be high enough to bind excess testosterone, preventing visible effects.
From 10 years of reproductive endocrinology consultation: I’ve diagnosed dozens of women with PCOS who were shocked because they “didn’t look or feel like they had it.” Their greatest challenge was taking the diagnosis seriously enough to implement preventive measures when they felt perfectly healthy.
How Is Asymptomatic PCOS Discovered?
Common discovery scenarios:
During fertility evaluation:
- Difficulty conceiving despite regular periods
- Ovulation tracking shows inconsistent or poor-quality ovulation
- Transvaginal ultrasound reveals polycystic ovaries
- Hormonal panel shows elevated LH/FSH ratio or high testosterone
Routine health screening:
- Annual gynecological exam includes pelvic ultrasound
- Blood work for other reasons reveals metabolic markers
- Family history prompts proactive PCOS screening
- Pre-conception health check identifies hormonal imbalances
Investigating subtle concerns:
- Unexplained weight gain despite no lifestyle changes
- Very mild thinning of scalp hair (often dismissed initially)
- Occasional long cycles (38-40 days) considered “normal variation”
- Skin tags or darkening in body folds (acanthosis nigricans)
Screening family members:
- Mother or sister diagnosed with PCOS prompts testing
- Genetic predisposition drives preventive screening
- Healthcare provider recommends testing based on risk factors
Diagnostic Tests That Reveal Silent PCOS
Essential diagnostic workup:
1. Transvaginal or abdominal ultrasound
- Counts follicles per ovary (12+ indicates polycystic morphology)
- Measures ovarian volume (>10 mL suggests PCOS)
- Best performed in early follicular phase (days 2-5 of cycle)
- 3D ultrasound provides more accurate assessment
2. Hormone blood tests (specific timing matters)
Day 2-5 of menstrual cycle:
- FSH (follicle-stimulating hormone)
- LH (luteinizing hormone) – elevated LH/FSH ratio suggests PCOS
- Testosterone (total and free)
- DHEA-S (dehydroepiandrosterone sulfate)
- Prolactin (to rule out other conditions)
- TSH (thyroid function—mimics PCOS symptoms)
Any time:
- Fasting insulin and glucose (insulin resistance assessment)
- HbA1c (long-term glucose control)
- Lipid panel (cholesterol, triglycerides)
- SHBG (sex hormone-binding globulin—low in PCOS)
- Anti-Müllerian hormone (AMH—typically elevated in PCOS)
3. Additional assessments
- Oral glucose tolerance test with insulin measurements
- Body composition analysis
- Blood pressure monitoring
- Liver function tests
Interpretation nuance: You can have “normal” testosterone (45 ng/dL in a reference range of 15-70) but still have PCOS if combined with polycystic ovaries and subtle ovulatory dysfunction. Context and combination matter more than single abnormal values.
Health Risks of Untreated Asymptomatic PCOS
Critical understanding: Lack of symptoms ≠ lack of risk.
Even without visible manifestations, PCOS creates significant long-term health vulnerabilities:
Metabolic complications:
- Insulin resistance: 50-70% of PCOS women develop this, even at normal weight
- Type 2 diabetes: 4x higher risk, often developing 10-15 years earlier than general population
- Metabolic syndrome: Cluster of conditions (high BP, abnormal cholesterol, increased waist circumference)
- Non-alcoholic fatty liver disease (NAFLD): 30-55% prevalence in PCOS
Cardiovascular risks:
- Higher triglycerides and LDL cholesterol
- Lower HDL (good cholesterol)
- Increased arterial stiffness and endothelial dysfunction
- 2-3x elevated risk of heart disease and stroke
- Higher prevalence of hypertension
Reproductive complications:
- Infertility: Even with regular periods, ovulation quality may be compromised
- Miscarriage risk: 30-50% higher than women without PCOS
- Pregnancy complications: Gestational diabetes, preeclampsia, preterm birth
- Endometrial cancer: 3x higher risk due to unopposed estrogen from irregular ovulation
Psychological impact:
- Increased rates of anxiety and depression (not just from visible symptoms)
- Body image concerns if weight gain develops
- Stress about fertility and long-term health
Research published in the Journal of Clinical Endocrinology & Metabolism demonstrates that metabolic complications develop regardless of symptom severity, making early intervention crucial even for asymptomatic presentations.
Why Early Detection Matters (Even Without Symptoms)
Benefits of diagnosing asymptomatic PCOS:
1. Prevent progression Early lifestyle interventions prevent insulin resistance from worsening and diabetes from developing. Studies show that losing just 5-7% of body weight (if overweight) significantly improves metabolic markers.
2. Optimize fertility Understanding PCOS before trying to conceive allows proactive ovulation support, reducing time to pregnancy and miscarriage risk.
3. Reduce cancer risk Regular periods or induced cycles with hormonal contraceptives protect endometrial lining from cancer-causing unopposed estrogen exposure.
4. Cardiovascular protection Managing cholesterol, blood pressure, and inflammation reduces heart disease risk that accumulates silently over decades.
5. Informed family planning Knowledge enables better timing and support for pregnancy attempts with appropriate medical guidance.
6. Empowered health decisions Understanding your diagnosis allows informed choices about diet, exercise, supplements, and medications before problems emerge.
What to Do If You Have Asymptomatic PCOS
Step 1: Confirm the diagnosis properly
- Ensure complete hormonal panel was performed at correct cycle timing
- Verify ultrasound was interpreted by experienced provider
- Rule out other conditions (thyroid disorders, hyperprolactinemia, congenital adrenal hyperplasia)
- Consider second opinion if diagnosis feels uncertain
Step 2: Establish baseline health metrics
- Complete metabolic panel (glucose, insulin, HbA1c, lipids)
- Blood pressure measurement
- Body composition analysis (not just weight/BMI)
- Liver function tests
- Cardiovascular risk assessment
Step 3: Implement lifestyle foundations
Nutrition strategies:
- Low-glycemic index diet to manage insulin
- Balanced macronutrients (40% carbs, 30% protein, 30% healthy fats)
- Anti-inflammatory foods (omega-3s, colorful vegetables, berries)
- Limit processed foods, added sugars, refined carbohydrates
- Consider Mediterranean or DASH diet patterns
Exercise protocol:
- 150+ minutes weekly of moderate aerobic activity
- 2-3 strength training sessions weekly (crucial for insulin sensitivity)
- High-intensity interval training (HIIT) 1-2x weekly if tolerated
- Daily movement and reduced sedentary time
Stress management:
- Chronic stress elevates cortisol, worsening insulin resistance
- Meditation, yoga, deep breathing exercises
- Adequate sleep (7-9 hours nightly—poor sleep worsens metabolic function)
- Mental health support if anxiety or depression present
Step 4: Consider medical interventions
For metabolic health:
- Metformin: First-line for insulin resistance prevention
- Inositol supplements: Myo-inositol and D-chiro-inositol improve insulin sensitivity
- Omega-3 fatty acids: Reduce inflammation and triglycerides
For cycle regulation and endometrial protection:
- Combined oral contraceptives: Regulate cycles, reduce androgen levels, protect endometrium
- Cyclic progesterone: Induces period every 3 months if not using contraceptives
For fertility when ready:
- Letrozole or clomiphene: First-line ovulation induction
- Assisted reproductive technologies: If first-line treatments unsuccessful
Step 5: Establish monitoring schedule
- Annual fasting glucose and HbA1c
- Annual lipid panel
- Blood pressure checks every 6 months
- Weight and waist circumference tracking
- Fertility assessment when planning conception
- Mental health screening annually
Lifestyle Modifications That Make the Biggest Difference
Evidence-based interventions for asymptomatic PCOS:
1. Weight management (if overweight) Even 5% weight loss dramatically improves:
- Insulin sensitivity (30-40% improvement)
- Ovulation regularity (increases by 50%)
- Androgen levels (decrease 20-30%)
- Cardiovascular risk markers
2. Resistance training (for all body types) Building muscle mass is the single most effective intervention for insulin resistance. Three weekly sessions of 30-45 minutes produce measurable metabolic improvements within 8 weeks.
3. Low-glycemic nutrition Choosing foods that don’t spike blood sugar prevents insulin surges that worsen PCOS:
- Swap white rice for quinoa or cauliflower rice
- Choose sweet potatoes over white potatoes
- Select steel-cut oats instead of instant oatmeal
- Pair carbohydrates with protein and healthy fats
4. Anti-inflammatory eating Chronic inflammation underlies many PCOS complications:
- Fatty fish 2-3x weekly (salmon, sardines, mackerel)
- Turmeric, ginger, green tea
- Colorful vegetables and berries
- Extra virgin olive oil
- Nuts and seeds
5. Supplement support Evidence-based supplements for PCOS:
- Inositol (4g daily): Improves insulin sensitivity and ovulation
- Omega-3s (2-3g daily): Reduces inflammation and triglycerides
- Vitamin D (2000-4000 IU if deficient): Improves insulin and reproductive function
- N-acetylcysteine (600mg 2x daily): Antioxidant supporting metabolic and reproductive health
- Magnesium (300-400mg): Supports insulin sensitivity and sleep
Special Considerations for Different Life Stages
Adolescence and young adulthood (15-25 years):
- Diagnosis challenging as irregular cycles normal post-menarche
- Focus on establishing healthy habits early
- Oral contraceptives often prescribed for cycle regulation
- Education about long-term implications crucial
Reproductive years planning pregnancy (25-40 years):
- Preconception counseling essential
- Optimize metabolic health 3-6 months before trying
- Folic acid supplementation (higher doses often recommended)
- Consider fertility evaluation if not conceiving within 6 months
Perimenopause and beyond (40+ years):
- Metabolic risks intensify with declining estrogen
- Cardiovascular screening becomes more critical
- Diabetes prevention remains paramount
- Hormone replacement therapy decisions require PCOS context
When to Seek Medical Attention Despite Lack of Symptoms
Red flags requiring immediate evaluation:
- Sudden menstrual cycle changes (previously regular becoming irregular)
- Unexplained rapid weight gain (>10 pounds in 3 months)
- New onset of excessive thirst or urination (diabetes warning)
- Development of acanthosis nigricans (dark, velvety skin patches)
- Difficulty conceiving after 6 months of trying
- Extreme fatigue or mood changes
- Family history of early diabetes or heart disease
Routine check-ins needed:
- Annual wellness visits with PCOS-informed provider
- Periodic reassessment of treatment plan effectiveness
- Pre-pregnancy planning consultation
- Mental health support as needed
Finding the Right Healthcare Provider
Ideal PCOS care team includes:
Primary provider options:
- Reproductive endocrinologist (hormonal expertise)
- Gynecologist with PCOS specialization
- Endocrinologist (metabolic focus)
- Informed primary care physician
Support specialists:
- Registered dietitian (preferably PCOS-specialized)
- Mental health professional
- Fertility specialist (when ready for pregnancy)
- Exercise physiologist or personal trainer
Questions to assess provider PCOS knowledge:
- “What are the Rotterdam criteria for PCOS diagnosis?”
- “How do you approach asymptomatic PCOS?”
- “What’s your philosophy on metformin for PCOS prevention?”
- “How often should I be screened for diabetes and heart disease?”
Providers who dismiss your concerns because you “look healthy” or “don’t have symptoms” may not be the right fit for managing a condition that requires proactive prevention rather than reactive symptom treatment.
Indian Context: PCOS Without Symptoms in Indian Women
Prevalence in India: PCOS affects 9.13-36% of Indian women depending on region and diagnostic criteria—among the highest rates globally. Genetic predisposition and dietary patterns contribute to high prevalence.
Unique considerations:
Higher metabolic risk: Indian women develop insulin resistance and diabetes at lower BMIs than Caucasian women. A BMI of 23-25 (considered normal internationally) carries increased risk in Indian populations.
Different symptom presentation: Some Indian women with PCOS have minimal hirsutism despite high androgens due to genetic factors affecting hair follicle sensitivity.
Diagnostic access:
- Ultrasound availability varies—urban areas have better access
- Hormone testing may be limited in rural settings
- Cost of comprehensive panel: ₹3,000-₹8,000 depending on city and facility
Cultural factors:
- Delayed diagnosis due to normalization of irregular periods
- Fertility concerns often drive diagnosis
- Family pressure around weight and appearance
Diet adaptations: Traditional Indian diets can be PCOS-friendly with modifications:
- Choose whole wheat roti over white rice
- Include dal/legumes for protein and fiber
- Use traditional spices (turmeric, fenugreek, cinnamon)
- Limit high-glycemic foods like maida products and sweets
Affordable interventions in India:
- Metformin is inexpensive (₹50-200/month)
- Inositol supplements: ₹800-1,500/month
- Lifestyle modifications cost-free or low-cost
FAQs
How common is PCOS without obvious symptoms?
Approximately 20-30% of women with PCOS have minimal or no obvious symptoms. The exact percentage varies based on which diagnostic criteria are used and population studied. Asymptomatic PCOS is most common in lean women and those with the ovulatory phenotype.
Can I have PCOS with completely regular 28-day cycles?
Yes. While irregular cycles are common in PCOS, regular menstruation doesn’t exclude the diagnosis. You can ovulate regularly but still have polycystic ovaries and hyperandrogenism. The ovulatory phenotype represents 10-20% of PCOS cases.
If I have no symptoms, do I really need treatment?
Yes. Treatment for asymptomatic PCOS focuses on preventing long-term complications like diabetes, heart disease, and endometrial cancer rather than managing current symptoms. Lifestyle modifications and potentially medications like metformin protect your future health even when you feel fine now.
Will asymptomatic PCOS make it hard to get pregnant?
Possibly. Even with regular periods, ovulation quality might be compromised, potentially extending time to conception. However, many women with mild PCOS conceive naturally. Informing your fertility specialist about your diagnosis enables appropriate monitoring and support if needed.
Can PCOS go away if I never had symptoms?
PCOS doesn’t truly “go away,” but its presentation can change across your lifespan. Symptom severity may fluctuate with weight changes, stress, and hormonal transitions. Even if asymptomatic now, monitoring remains important as risks persist throughout life.
Should my daughter be tested if I have asymptomatic PCOS?
PCOS has strong genetic components—first-degree relatives have 30-40% chance of having it. Consider screening your daughter in late adolescence (2-3 years post-menarche) if she shows any subtle signs, or proactively in her early 20s given your diagnosis.
Is asymptomatic PCOS easier to treat than symptomatic PCOS?
Not necessarily “easier,” but the treatment goals differ. You’re working on prevention rather than symptom relief, which can actually be more challenging because you won’t feel immediate benefits. The motivation must come from understanding long-term health protection rather than symptom improvement.
Can birth control pills mask PCOS symptoms and prevent diagnosis?
Yes. Oral contraceptives regulate cycles and reduce androgens, potentially hiding PCOS symptoms. If PCOS is suspected, testing should occur after stopping birth control for 3 months (under medical supervision) to see your body’s natural hormonal pattern.
What’s the difference between polycystic ovaries and PCOS?
Polycystic ovaries are a structural finding on ultrasound (multiple small follicles creating a specific appearance). PCOS is a syndrome involving hormonal, metabolic, and reproductive dysfunction. About 20-30% of healthy women have polycystic ovaries without having PCOS syndrome.
Conclusion
The question “Can I have PCOS but not have any symptoms?” has a definitive answer: absolutely yes. Asymptomatic or silent PCOS affects an estimated 20-30% of women with the condition, challenging the stereotype that PCOS always announces itself through irregular periods, unwanted hair growth, stubborn weight gain, or persistent acne.
Your lack of obvious symptoms doesn’t diminish the validity of your diagnosis or the importance of taking it seriously. PCOS without symptoms still carries significant long-term health risks—insulin resistance, type 2 diabetes, cardiovascular disease, and endometrial cancer don’t require visible manifestations to develop silently over decades.
The advantage of discovering asymptomatic PCOS early is the opportunity for prevention rather than damage control. Through evidence-based lifestyle modifications—low-glycemic nutrition, regular resistance training, stress management, and strategic supplementation—you can dramatically reduce your risk of developing metabolic complications. When appropriate, medical interventions like metformin, inositol, or hormonal contraceptives provide additional protection.
Regular monitoring through annual metabolic panels, cardiovascular screening, and reproductive health assessments ensures complications are caught early if they do develop. Working with a PCOS-informed healthcare provider who understands that “feeling fine” doesn’t mean “nothing to address” makes all the difference in long-term outcomes.
Now you understand that PCOS exists on a spectrum, that your asymptomatic presentation is valid and requires attention, and that proactive management today protects your metabolic, cardiovascular, and reproductive health for decades to come—even when you can’t see or feel what’s happening beneath the surface.